
COVID and Hearing Health
Most otolaryngologists will agree that hearing complaints are on the rise this past year – whether it’s sudden hearing loss, new onset sensory hearing loss, and new or worsening tinnitus (ringing in the ears). We have seen these complaints during and following a confirmed COVID-19 infection, as well as seemingly on the rise following the mRNA COVID vaccinations.
We have long known that various upper respiratory viruses can affect the hearing and balance nerves, causing a virally induced nerve hearing loss (sensorineural hearing loss). Certainly with all of the health implications of Sars-COV2 Coronavirus infection we are sure to see similar symptoms in various cranial nerves (smell being the most publicized). To date, no large-scale scientific evaluation has been completed on the incidence of hearing loss with COVID-19 – We have merely a collection of anecdotal reports of spikes in hearing loss complaints.
Hearing loss is sometimes very easy to understand – feeling like we cannot hear in one ear. When there is isolated middle or high frequency hearing loss though, many patients will simply feel like they are ears clogged or stuffed up or perhaps full of fluid. Also sometimes ear diagnosis can be very difficult at various walk-in clinics or by telemedicine, since some patients are lead to believe that they may have simple fluid in the ear or allergies causing hearing loss. Many of these patients turn out to have a new onset nerve based hearing deficit that simply feels like stuffiness to them.
Hearing loss may also manifest only as ringing in the ear, feeling as though there is an overwhelming buzzing or ringing that is blocking all hearing.
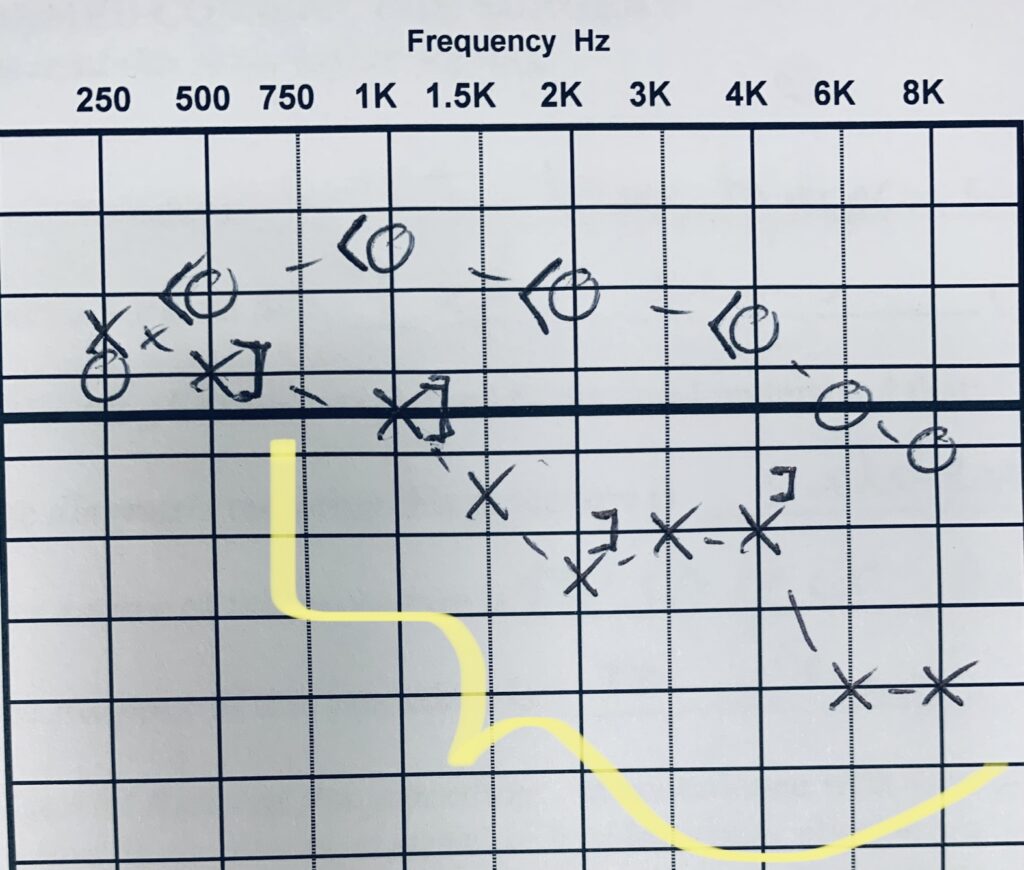
 A good objective evaluation of hearing loss as needed. Most otolaryngologists, including Advanced ENT, employ Doctoral audiologists (Au.D) to perform a thorough acoustic nerve analysis. This will typically include a full audiogram with or without extended spectrum, distortion product otoacoustic emission testing, as well as tympanometry. We also will test speech discrimination scores to see if central understanding has been impaired. Testing for tinnitus is a bit more tricky. The audiogram is taken in context with the various severity indexing surveys that can be done in the office.
A good objective evaluation of hearing loss as needed. Most otolaryngologists, including Advanced ENT, employ Doctoral audiologists (Au.D) to perform a thorough acoustic nerve analysis. This will typically include a full audiogram with or without extended spectrum, distortion product otoacoustic emission testing, as well as tympanometry. We also will test speech discrimination scores to see if central understanding has been impaired. Testing for tinnitus is a bit more tricky. The audiogram is taken in context with the various severity indexing surveys that can be done in the office.If you have developed worsened hearing or tinnitus in this past year it is probably worthwhile getting a good evaluation. It is very tough for automated audiology equipment to get a good specific evaluation, usually those tests will result more and a passive/fail result and will miss subtle findings. Hearing loss that is sudden in onset, or tinnitus or fullness that is sudden in onset should be evaluated ASAP. Many of these can be reversed by appropriate medical management if done soon enough.
When we do see hearing loss or tinnitus that is new in onset, or particularly if if the hearing change is asymmetrical between the sides, we usually recommend some form of central imaging such as specialized MRI series. This ensures that were not dealing with more concerning brain problem such as a meningioma, acoustic neuroma, multiple sclerosis or even stroke.
Good evaluation of new onset hearing loss, ear pressure, ear fullness, or feeling stuffy in the should be visit in person by an otolaryngologist (ear nose & throat doctor), as well as a good hearing test report from an audiologist. Let us know how we can help — we see these kinds of hearing problems every day!